Edited by:

Reasoning behind early Aquatic Therapy intervention may be found to be unclear for many healthcare professionals. As testified during the latest podcast by Eugenia Hernàndez, clinical evidence is extremely hard to produce because of the large spread in pre-existing conditions of patients the are treated in the pool. Even evidence based proof is hard to quantify, but has clearly been qualified. At the same time Roel van Oorsouw (ICU Physio Therapist at Radboud UMC) reports patients, and their families get a huge boost from the Aquatic Therapy intervention. After the treatment, patients “sleep like babies”, which might point into the direction that important physiological processes have commenced as a result of the intervention.

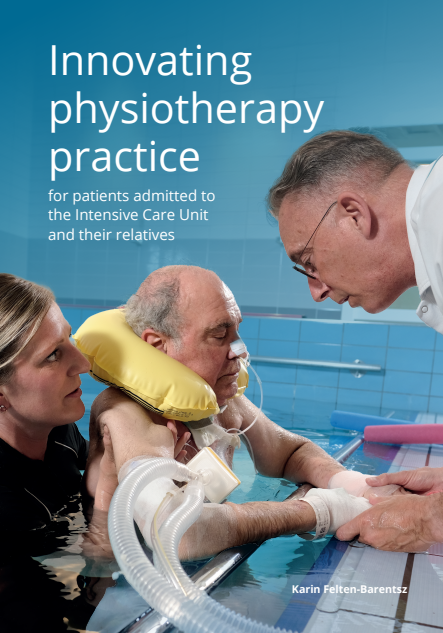
Roel van Oorsouw works right on the frontline, with patients which have been on a ventilator for prolonged periods of time, using Aquatic Therapy as an early intervention to build up muscle tissue and relearn motor control. As a result of the inspired conversation during the podcast, Johan Lambeck (IATF Senior Lecturer), has endeavoured to write a short article about the untold story about early Aquatic Therapy intervention in post-ICU patients. We would like to share this short article underneath:


Disembodyment
Aquatic physical therapy at an intensive care unit (ICU) is rare. But the ICU at the university hospital RadboudUMC in Nijmegen, Netherlands, has a pool since 2012. The reason is to help with recovery of e.g. critically ill ventilated patients in a very early stage, also for patients with serious complications of Covid-19. Therapists not only aim to treat the physical effects of intensive care unit acquired weakness (a part of the post intensive care syndrome), but also aim to positively affect control, hope and trust. This combination of goals comes from the embodiment paradigm.
At its heart, embodiment emphasizes an orientation towards the whole person (an attitude towards the full richness of human life), and a rejection of singular, reductionistic views of the body common to the biomedical sciences (from Nicholls 2010). Embodiment is also defined as being specifically concerned with the lived experience of one’s own body. This lived experience refers to the way that individuals negotiate their everyday lives via the utility of their bodies, and how they mediate, interpret, and interact with their physical and social environments. Embodiment is about the implicit/tacit functioning of the body in everyday perception and performance. Body, mind, action, and perception are a unity in this concept, influenced by e.g. Merleau-Ponty (1962).
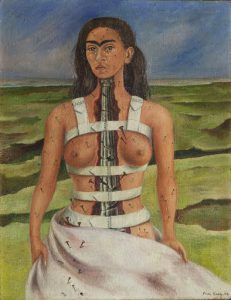
Merleau-Ponty described the “basic sense of self”: the “mineness” of all experiences, embedded in a background feeling of the body in terms of “my experiences are my own”. The “mineness of acting” is the experience of the one who – spontaneously – initiates action. Disembodiment is the disturbance of this implicit functioning. Disability can disembody, as wonderfully has been painted by Frida Kahlo in her “The Broken Column”. The hemiplegic neglected arm can be disembodied, or the fractured leg as described by Oliver Sacks in “A leg to stand on”. Disembodiment also exists in the ICU: life is at stake and the normal body becomes an infarcted heart that is monitored in various ways with an abundancy of equipment. To align body, mind and action again, a person has to relearn that “my bodily experiences are my own” through sensorimotor (movement) experiences in combinations with emotions and behaviour.
Practically: a person needs the experience that the body can perform and can be controlled. Aquatic therapy facilitates this: slow movements or maintaining a posture only need some 5% of maximum strength (on land this is about 20%). This helps embodiment also through the model of self-efficacy: belief in one’s own capabilities (yesss, in the pool I can already make a few steps; I will also be able to do that on land at some moment: possibly providing a turning point in my recovery). Training weakness is a fight against gravity. Buoyancy during immersion counteracts gravity and depends on the amount of immersion (volume displacement). Progression in training needs a gradual increase of gravity, which is realized by the adjustable floor.
** not every patient can go into the pool. There are in/exclusion criteria. Specific for Covid-19: 3 negative tests.
Otherwise the criteria are related to circulation and respiration:
Patient does not fulfill vital functions safety criteria:
- Respiratory instability
– Inspiratory oxygen fraction (FiO2) > 60%
– Positive end expiratory pressure (PEEP) > 10 cmH2O
– Frequent desaturation < 90%
– Breath rate > 40/min - Hemodynamical instability
– Mean arterial pressure (MAP) < 65 mmHg (norm value 65-110)
– new myocardial ischemia * serious arrhythmia’s - Neurological instable
– Intracranial pressure (ICP) > 15 mmHg (norm value 7-15) - Other
– Fever > 400 C / 1040F
– active bleeding
– serious agitation: Richmons Agitation Sedation Scale (RASS) +1 till +4
– thrombocyte count < 10 (*103/ml)
– unsafe endotracheal tube
Video’s
These news items include video’s of aquatic therapy and of COVID -19 in RadboudUMC:
Video Dutch National TV (in Dutch)
References
Felten-Barentsz KM, Oorsouw van R, Haans AJC, Staal B, Hoeven van der JG, Nijhuis-van der Sanden MGW. Patient views regarding the impact of hydrotherapy on critically ill ventilated patients: A qualitative exploration study. Journal of Critical Care, 2018; 48: 321–327. https://doi.org/10.1016/j.jcrc.2018.09.021
Jaye C. Talking around embodiment: the views of GPs following participation in medical anthropology courses. J Med Ethics; Medical Humanitie,s 2004. doi: 10.1136/jmh.2003.000146
Martin LAL, Koch SC, Hirjak D, Fuchs T. Overcoming disembodiment: The effect of movement therapy on negative symptoms in schizophrenia—A multicenter randomized controlled trial.. Frontiers in Psychology, 2016. doi: 10.3389/fpsyg.2016.00483
Merleau-Ponty M 1962 Phenomenology of perception (C. Smith,Trans.). New York, Humanities Press
Nicholls DA, Gibson BE. The body and physiotherapy. Physiotherapy Theory and Practice, 2010;26(8):497–509. DOI: 10.3109/09593981003710316
Schaffeld S (2019). Ambiguity, the disembodied self, and the performative How medical imaging techniques inform embodied art-work Introduction. https://www.researchgate.net/publication/337335164